Dr Taylor also regularly performs other keyhole surgeries including removal of the Gallbladder, hernia repair, and Reflux/Hiatus Hernia surgery. Call us for further details or to make an appointment.
Gallbladder
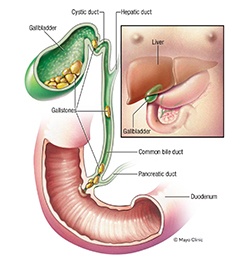
The Gallbladder is a pear-sized organ attached to the underside of the liver used to store bile. Bile is needed for the digestion and absorption dietary fats. Contrary to popular belief, bile is not made in the gallbladder, but is instead made by the liver, and flows into the intestine via the bile duct. The gallbladder simply stores the bile between meals. This storage need is not particularly relevant anymore in modern life- it is an ancient carry over from the caveman era, during which humans were hunter-gatherers and may not eat for several days at a time. The ability to store bile was therefore important. However in modern life where we eat several times every day, we no longer need a gallbladder to store bile between meals.
In approximately 20% of people stones form within the gallbladder. This risk is even higher, up to 30%, in people with obesity, females, or those with a family history. Stones form when the ratio of the chemical components in bile, including Lecithin, cholesterol, bile salts, and bilirubin, fall out of the correct proportions. Gallstones range in size from as small as a grain of sand to as large as a golf ball. Some people develop just one gallstone, while others develop many gallstones at the same time.
Stones cause irritation to the lining of the gallbladder, called chronic cholecystitis, which can make people feel tired and run down. They can also temporarily block the neck of the gallbladder, causing acute pain called biliary colic. This is most likely to occur after a meal. Biliary colic is an unpleasant sudden and rapidly intensifying pain in the centre of your upper abdomen, going through to the back or right shoulder, and is frequently associated with nausea.
Gallstones can also lead to more serious problems that may require urgent hospitalisation: If the stone remains impacted in the gallbladder neck for more than a few hours the gallbladder becomes swollen and infected, a condition called acute cholecystitis. If gallstones migrate into the bile duct they can cause jaundice, or block the pancreatic duct and lead to pancreatitis.
Whilst various remedies to try and dissolve gallstones have been tried over the years, all have failed. Surgical removal of the gallbladder is the only effective treatment of gallstones, and is recommended if you have symptomatic gallstones. The gallbladder is removed by laparoscopic keyhole surgery. This involves 4 small incisions under a general anaesthetic, and takes approximately one hour. The gallbladder is retracted to expose the cystic duct and artery which are clipped and divided before removing the gallbladder. An X-ray of the main bile ducts (an intra-operative cholangiogram) is usually performed at the same time to check if any stones have become lodged in the bile duct. The procedure is quick and safe, with a 1- 2% risk of complications. It involves an overnight hospital stay, and 5-7 days off work.
Hernia
A hernia is a protrusion, usually of either abdominal fat or intestine, through a weakened area of the abdomen wall or groin. They are usually noticed as a lump that enlarges when standing or straining. Because hernias may contain abdominal contents such as intestine they must be repaired to prevent incarceration and strangulation. A hernia will not get better by itself, and must be repaired surgically.
Nowadays hernias are repaired using laparoscopic keyhole surgery. This involves three small incisions on the side of the abdomen to access the area of weakness from below. The hernia is pulled back, and the weakness strengthened by inserting a sheet of mesh. Connective tissue (collagen) ingrowth into the mesh then takes place over the following 8 weeks, incorporating the mesh into the back of the abdominal muscle. The repair becomes mature and strong once the mesh has become fully incorporated into the abdominal wall. The procedure involves an overnight hospital stay, and 5-7 days off work. Strenuous physical activity should be avoided for 6 weeks.
Hernia Types
There are different types of hernias depending on their location. The most common types are:
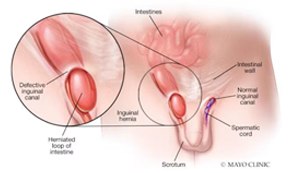
- Inguinal Hernia: Appears as a bulge in the groin or scrotum, occurring more commonly in men than women. Inguinal Hernias are one of the most common types of hernia, and can occur in all age groups. There are two types; Direct and Indirect. Direct hernias bulge through a weakness in Hasslebachs triangle just above the pubic bone. Indirect hernias go through the inguinal canal alongside the spermatic cord (or round ligament in females). Both types are repaired in the same manner- the hernia is repaired from the inside with mesh using laparoscopic surgery.
- Femoral Hernia: A femoral hernia appears as a bulge in the inner aspect of the upper thigh or groin. This type of hernia tends to occur in older people and is more common in women than in men. Because the edges of the hernia defect are hard, the contents usually become incarcerated, and must be repaired straight away especially if there is any intestine involved.
- Umbilical Hernia: An umbilical hernia is a common hernia presenting as a small bulge coming out of the umbilicus (belly button). They may be due to incomplete closure of the muscles around the umbilicus during infancy, but more commonly develop in later years due to the inherent weakness in the umbilical area. If very small they can be repaired with a simple suture, however medium and large umbilical hernias are repaired with mesh using laparoscopic surgery.
- Hiatus Hernia: A hiatus hernia is when part of the stomach organ slides through the hiatus opening in the diaphragm (the muscular sheet that separates the chest from the abdomen and is responsible for breathing). The most common way hiatus hernia’s present is with reflux or regurgitation, because the reflux valve at the bottom of the oesophagus no longer works effectively. Hiatus Hernias may also cause swallowing problems due to distortion of the food pathway from oesophagus to stomach. Hiatus hernias are an exception to the general rule in that they are usually not repaired with mesh. Instead they are repaired by performing a fundoplication using laparoscopic surgery.
- Incisional Hernia: An incisional hernia is a hernia protruding through the muscle layer of an old surgical incision on the abdomen. The lump will be underneath the old scar.
- Parastomal Hernia: this hernia is one that occurs alongside a colostomy or ileostomy. They can cause problems with the proper emptying of the stoma, and can be rather tricky to deal with.
Reflux Surgery
Gastro-oesophageal Reflux Disease (GORD) occurs when fluids in the stomach (a mixture of acid, pepsin, and bile) travel back into the oesophagus because the anti-reflux valve is not working properly. It is normal for some reflux- up to 4% of the time- but as these reflux fluids are quite corrosive to the lining of the oesophagus, any exposure longer than this can cause damage. The oesophageal lining can become inflamed (oesophagitis) and develop ulcers. Patients with reflux commonly experience heartburn, which is a burning feeling behind the breast bone, that often feels like it is rising up. It is most commonly experienced after eating certain foods such as spicy food and alcohol, or when lying down at night.
In more severe cases, the reflux fluids can rise up to the throat and cause chronic cough, voice hoarseness, dental decay, and even pneumonia. Over time, chronic inflammation can lead to adaptive responses by the cells that line the oesophagus, which undergo changes to better withstand the constant exposure to corrosive fluids. Unfortunately these changes, known as Barretts oesophagus, can trigger a cascade towards cancerous growth.
Treatment of GORD is dependent upon its severity. In mild and occasional cases, this starts with simple measures such as avoidance of precipitating foods, not eating close to bed time, neutralising antacids, and sleeping with the head of the bed propped up. Where symptoms are occurring on a daily basis, acid suppression medications such as Losec, Somac, Nexium or Pariet are often used. However whilst these medications are useful for reducing acid production by the stomach, they do not reduce the other fluids often found in reflux such as pepsinogen or bile. And they do not improve the functioning of the faulty anti-reflux valve. There is also growing concern that long term use of these medications can accelerate osteoporosis, and also cause reduced Iron and Vitamin absorption.
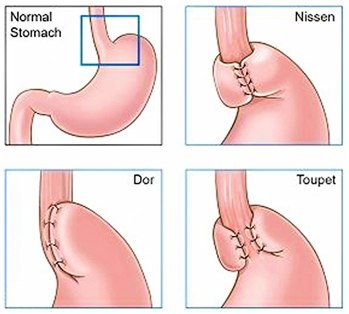
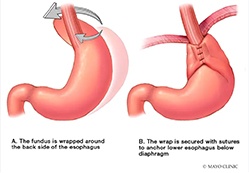
Surgery for reflux is all about improving the way the valve functions between the stomach and oesophagus. During the surgery, which is performed laparoscopically, the lower third of the oesophagus is mobilised, and the valve brought down into the abdomen. The external part of the valve, the crural pinch, is tightened with sutures. A fundoplication is then performed which further enhances the effectiveness of the valve repair. The procedure typically takes one hour, and requires just a one night stay. Patients are able to mobilise and drink a wide variety of fluids immediately, and return to driving and gentle everyday life after about 3 days. Following surgery, the vast majority of patients report either significant improvement or complete resolution of their reflux symptoms, and can come off medication.
One of the unwanted side effects of tightening the valve too much can be gas bloating. Another potential side effect is difficulty swallowing tougher things like steak and bread. These issues can be troublesome in up to 10% of patients with the classic Nissen Fundoplication. As a result, we prefer to use a type of partial fundoplication called the Toupet, in which the fundoplication wraps around the back and sides of the oesophagus but not the front wall. This still provides excellent reflux control but has less issues with gas bloating or swallowing problems.